

Abstract

INTRODUCTION
Essential thrombocythemia (ET) is a classic Philadelphia chromosome-negative myeloproliferative neoplasm with low progression rate to secondary myelofibrosis and transformation to acute leukemia. Patient survival is prolonged and the main clinical focus in ET patients is prevention of thrombotic and hemorrhagic complications. Chronic inflammation may be one of the main reasons for progression and complications in ET. The somatic JAK2 V617F mutation found in about half of the patients with ET is associated with dysregulation and overexpression of inflammatory genes resulting in massive production of cytokines and other inflammatory mediators.
In spite of knowing that chronic inflammation is an important risk factor for the development of atherosclerosis in patients with chronic inflammatory diseases, such as rheumatoid arthritis, type 2 diabetes mellitus and systemic lupus erythematosus no clinical study has been published in patients with ET about deterioration of arterial function. Therefore, we tested patients with JAK2 V617F positive ET in comparison with age-and sex-matched, apparently healthy control subjects whether they show more advanced progression of arterial stiffness and pulse-wave velocity - parameters that increase with age and are associated with adverse cardiovascular outcomes.
PATIENTS AND METHODS
Thirty six patients with JAK2 V617F positive ET, without clinically apparent atherosclerotic disease and 38 apparently healthy individuals were enrolled in our study after giving their informed consent. The 10-year risk for coronary disease was assessed at inclusion by the Framingham risk equation. All subjects underwent two separate clinical visits for ultrasound examination of the extracranial carotid arteries (using Aloka prosound α7, Hitachi Aloka Medical, Ltd., Japan). Echo-tracking of the common carotid arterial wall 2 cm proximal to the bulb was used to assess the β-stiffness index and to estimate the pulse wave velocity. The first measurement was done between January 2014 and August 2015 and the second 3-4 years later between January and July 2018. Continuous variables were tested for normality and are presented as median values and inter-quartile range (QR) or mean values and standard deviation (SD). The differences between groups were evaluated either by the Mann-Whitney test or the Student's t-test for continuous data, or by the chi-square test for the sex distribution.
RESULTS
Patients with ET and control subjects did not differ in age and sex distribution (age at inclusion 57.5 (QR 45.8 - 64.9) vs 59.2 (QR 53.6 - 67.8) years, p = 0.17, male/female 12/24 vs. 14/24, p = 0.76) or in the predicted 10-year risk of coronary disease by the Framingham equation (6.84 (3.27-11.82) vs. 7.20 (3.61-10.37), p = 0.87) at inclusion in the study.
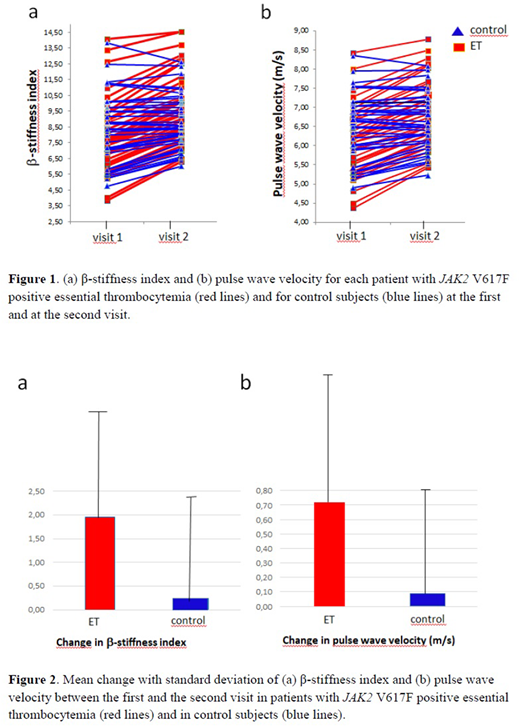
The mean β-stiffness index for patients with JAK2 V617F positive ET was 7.71 (standard deviation (SD) 2.42) at the first visit and 9.67 (SD 2.31) at the second visit, while the mean β-stiffness index for control subjects was 8.73 (SD 2.77) at the first visit and 8.97 (SD 1.91) at the second visit. Individual pairs of data are shown in Fig 1a. The increase in β-stiffness index between the first and the second visit for patient with JAK2 V617F positive ET was 1.95 (SD 2.17) and for control subjects 0.24 SD (1.96), p < 0.001 (Fig. 2a).
The mean pulse wave velocity for patients with JAK2 V617F positive ET was 6.20 m/s (SD1.04 m/s) at the first visit and 6.92 m/s (SD 0.93 m/s) at the second visit, while in control subjects it was 6.57 m/s (SD 1.00 m/s) at the first visit and 6.66 m/s (SD 0.79 m/s) at the second visit. Individual pairs of data are shown in Fig 1b. The difference in pulse wave velocity between the first and the second visit for patients with JAK2 V617F positive ET was 0.72 m/s (SD 0.92 m/s) and for control subjects 0.09 m/s (SD 0.71 m/s), p < 0.001 (Figure 2b).
CONCLUSIONS
Patients with JAK2 V617F positive ET had accelerated progression of arterial stiffness of the carotid arteries and estimated pulse wave velocity in the 3-4 year observation period compared with control subjects matched for age, sex and Framingham cardiovascular risk score.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal